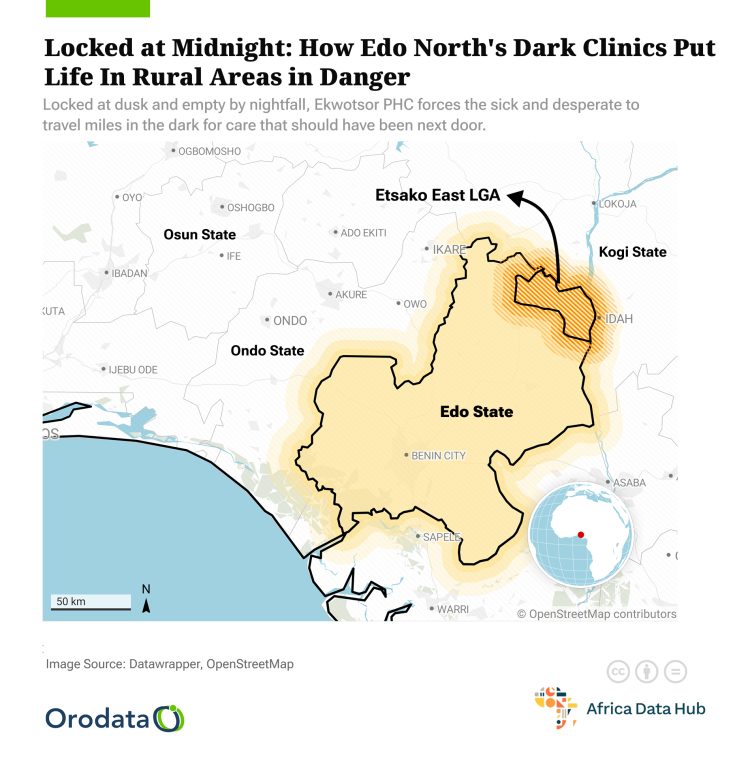
At exactly 1:30 a.m. in the remote community of Ekwotsor, Etsako East Local Government Area of Edo State, 27-year-old Aisosa Igbinovia frantically knocked on the entrance of the the Primary Health Centre (PHC) in the community, hoping to get help for her mother who had collapsed after hours of vomiting and weakness.
There was no answer. The centre, like many others in rural Edo, was closed.
“I called the nurse who works here, and she said she was in Agenebode (a 30-minute drive away). I had no choice but to put my mother on a bike to the General Hospital,” Igbinovia recounted.
Her experience is not an isolated one. Across rural communities in Edo North, particularly in places like Ekwotsor, Iviukwe, Ivianokpodi in Etsako East, and Eware and Ughiole-Aviele, Etsako West, residents are increasingly finding themselves in peril during health emergencies at night.
Primary health centres close at dusk and open at dawn due to poor staffing, absence of habitable staff quarters, and lack of operational support to run a 24-hour service.

While many of these PHCs boast of modern buildings—often products of donor or state-supported capital projects, the absence of staff at critical hours exposes a deep failure in health systems planning.
In Ivianokpodi, the PHC has a maternity ward, consulting rooms, but community members say the facility is effectively non-functional beyond 5:00 p.m.
“We have a nurse who comes during the day, but she goes back to Agenebode at night. The quarters built here are broken, no electricity, no water. No one wants to sleep here,” said Mr. Emmanuel Oboh, a local youth leader.
In Iviukwe, a farmer, Mrs. Elizabeth Udezwe shared how her pregnant daughter went into labour at 11:00 p.m. and was carried on by neighbours across kilometers to a private clinic in Fugar, a closeby semi-urban community.
“We could not even think of going to the PHC. It was locked, and we didn’t know where the nurse was,” she said.
This service gap is not from a lack of investment—at least on paper. In the Edo State 2024 approved budget of N485 billion, the health sector received N33.6 billion, out of which the Edo State Primary Healthcare Development Agency (EDSPHCDA) was allocated N5.4 billion.
However, an overwhelming N5.2 billion of this went into personnel expenditure, leaving little or no room for capital spending to renovate staff quarters, provide power, or build accommodations that would keep health workers in the communities they serve.
Even more concerning is that there was no specific capital expenditure line item for the agency in that year’s budget, and it remains unclear whether any PHC-related capital projects were folded into the Ministry of Health’s N19 billion capital allocation.
In 2025, the figures rose. The Ministry of Health was allocated N82.8 billion, with N8.4 billion earmarked for the Primary Healthcare Agency. Yet again, there was no mention of a capital expenditure provision under the agency’s line item, despite a staggering N56.5 billion capital vote for the ministry as a whole.
“Budget transparency and targeted spending remain key concerns. If PHCs are to operate round-the-clock, we need capital allocations that reflect their infrastructure needs, such as accommodation, electricity, and security.
“Otherwise, we are just paying salaries without service,” said Dr Igbineka Igbinedion, a health economist at the Edo State University.
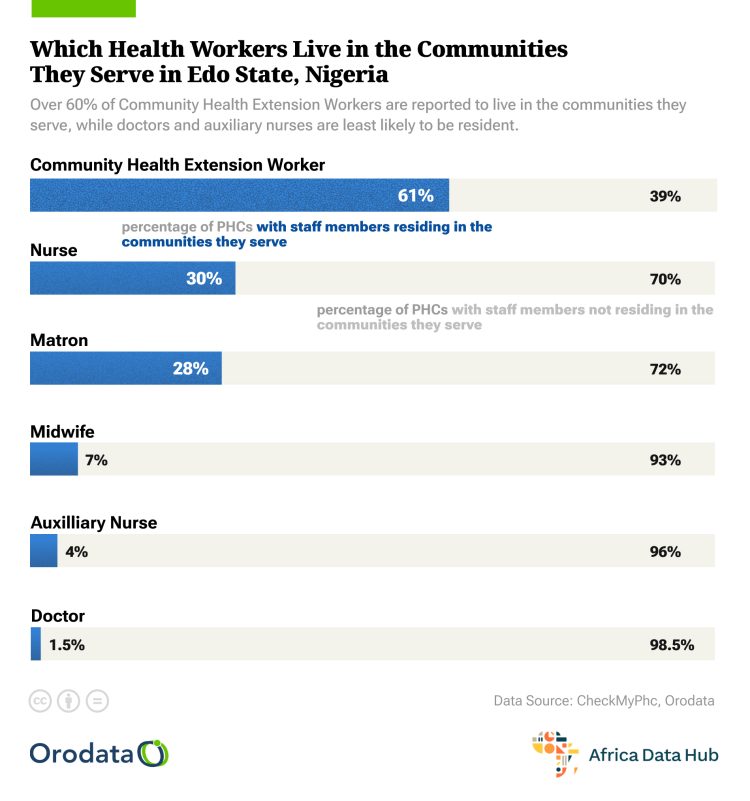
PHC staffing in rural areas presents a complex problem. Many health workers posted to remote towns do not reside in them. Instead, they commute daily from semi-urban centres like Auchi, and Agenebode, often leaving by 4:00 p.m. to avoid traveling after dark.
In Ughiole-Aviele, the community’s PHC sees fewer than three health workers per shift, and no one lives on-site. The staff quarters have leaking roofs and cracked walls.
“No one should live in that place. During the rains, it floods,” said one health worker who asked not to be named.

Eware faces a similar crisis. “The staff here leave before sunset. If anything happens at night, we know we are on our own,” said Mrs. Bridget Otaru, a traditional birth attendant.
In her 60s, she remains the unofficial night-time health responder in her village, relying on herbal remedies and home care. “I am not a trained nurse, but what do we do when the PHC is locked?”
Nigeria’s commitment to Universal Health Coverage (UHC) hinges largely on a functional and reliable PHC system, especially in rural areas where tertiary and secondary hospitals are scarce.
According to the National Primary Health Care Development Agency (NPHCDA), over 70 per cent of Nigerians rely on PHCs for basic health needs.
In Edo State, the push toward revitalising PHCs began under the Basic Health Care Provision Fund (BHCPF), aimed at financing essential services and reducing maternal and child mortality. But without staff accommodation and operational support, the initiative risks becoming another policy with poor rural impact.
“Healthcare is not just about erecting buildings. It’s about people, systems, and service availability. If staff cannot live where they work, the facility might as well not exist,” said Mr. Andrew Ugiagbe, a community health mobiliser in Etsako West.

He noted that the state has done well in partnering with development agencies for physical rehabilitation of PHCs but failed to address sustainability.
“You can’t expect a nurse to stay in a community with no light, no clean water, and no security. These are the basics,” he said.
The National Health Policy emphasises 24-hour PHC services as the frontline defense against preventable deaths. Yet, in Etsako East and West, this ideal remains far from reality. According to NHMIS data from 2023, Etsako East LGA recorded one of the highest rates of night-time emergency referrals in Edo North, primarily due to PHC closures.
Healthcare advocates in Edo are calling for immediate and deliberate action to address the deepening crisis in rural primary healthcare. They emphasise the urgent need to renovate and provide habitable staff quarters so that healthcare workers can reside within the communities they serve.
Without this basic provision, the idea of round-the-clock service remains unattainable. There is also a growing demand for a more transparent and intentional budgetary process—one that includes specific capital expenditures targeted at the Primary Healthcare Agency, rather than burying such needs within the broader Ministry of Health allocation.
In addition, health workers in rural areas should be incentivised through allowances, housing support, and career progression opportunities, to encourage them to stay and serve in these underserved locations.
Equally critical is the involvement of local communities in monitoring and supporting health facilities, fostering accountability and shared responsibility in maintaining continuous healthcare delivery. Mrs. Beatrice Aigbe, a midwife who has served in multiple rural PHCs across Edo North, summed it up poignantly:
“The communities want to help, but the state has to make it viable for workers to stay. Give us light, clean water, and pay attention to rural health needs. Otherwise, we’re wasting lives.”
As the sun sets over Edo North’s rural towns, the locked gates of primary healthcare centres become more than just physical barriers, they stand as stark symbols of a broken system that retreats when people are most vulnerable.
Behind each gate is a story of loss, a cry for help unanswered, and a life that might have been saved if the system stayed awake through the night. Until urgent reforms are made, stories like Aisosa’s will continue to echo in these quiet communities, poignant reminders of the cost of neglect in the face of preventable tragedies.
This story was produced for the Frontline Investigative Programme and supported by the Africa Data Hub and Orodata Science.